
A silver-bullet to save everything, or at least healthcare
Uncle Sam's Immigrant Nursing Brigade may hit a snag, but Random Walk has a solution

the deficit-funded-healthcare-driven-foreign-born growth story, for the uninitiated
the biggest policy change of the new admin, by far
hiring, healthcare, and visa support, like peas in a pod (an arb on the high barriers to entry)
the healthcare worker shortage, returns?
a radical YIMBY solution
👉👉👉Reminder to sign up for the Weekly Recap only, if daily emails is too much. Find me on twitter, for more fun. A silver-bullet to save everything, or at least healthcare
There are no silver bullets, but sometimes we can get close.
The closest thing to a “silver bullet” policy change would be to deregulate unthrottle healthcare completely. Random Walk calls it Healthcare Yimbyism. It’s unlikely to happen, but that doesn’t make it any less true.
When I say “completely,” I mean completely. I’d allow perhaps some bare requirements, like “register with the state and post a $50,000 bond,” but otherwise, everything goes, from provider, to insurance, to medicine, to medical devices, to snake oil—just let freedom reign, and caveat emptor.1
Among other reasons, liberating healthcare from state control would alleviate our most pressing economic issue: meeting the steady increase in demand for healthcare (and healthcare workers) without going bankrupt.
Let me explain.
Healthcare makes all the jobs (bc obviously, and now everyone concedes the point)
First, some context (but for the initiated, feel free to skip).
Look, it’s no secret now that national aging (which is a combination of time + failure to babymake) has both increased demand for healthcare goods and services, while (at the same time) depleting the number of people available to do the work.
Even the NYT is noticing the Rotation to the National Nursing Home:
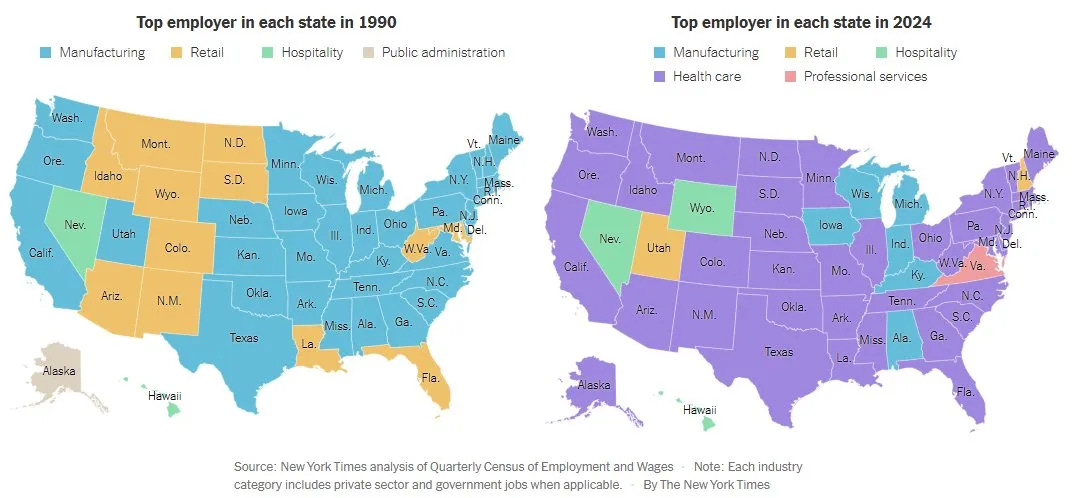
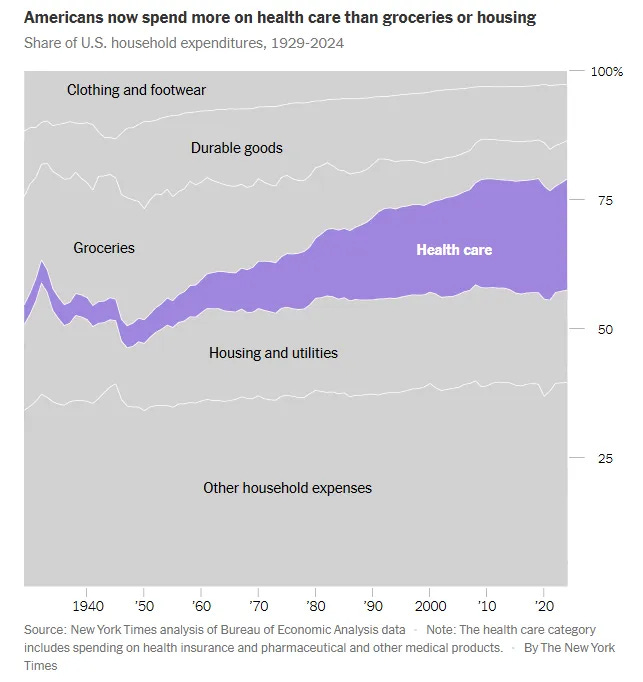
Healthcare is an increasingly large share of household consumption, and healthcare has become the dominant employer for most of the country.
Why has that happened? Again, mostly because we got older, and we’re rich.
In all events, the result is that over the last 50 years, we basically offset the decline in manufacturing jobs, with the growth of healthcare jobs.
Now, a good chunk of that additional marginal demand was met by women entering the workforce. No problem. But, again, as more people age-out of the workforce (with fewer reinforcements behind them), that means even more older folks to take care of, and even fewer people to do the work.
More work and fewer people is a problem.
So, we increasingly turned to “foreign born” workers (particularly foreign born women workers) to meet our insatiable demands for healthcare—literally ‘insatiable’ in the sense that we gave seniors the company card to expense all of this, so they keep buying because someone else is paying. But also, the healthcare-driven economy, became a healthcare+immigration driven economy. Random Walk is wont to call it Uncle Sam’s Immigrant Nursing Brigade.
In that regard, “foreign-born” workers are not just all the worker-growth, but they’re deflationary too. If demand is insatiable, but supply stayed relatively flat, then prices would go something-something.2
Put it all together, and it’s not an exaggeration to say (for better and for worse) that our “growth story” is (slowly, slowly, then quickly all at once) ‘we’re borrowing a lot of money to pay immigrants to take care of us in our old age.’ I mean, if [deficit-funded] healthcare makes all the jobs, and job growth is a foreign-born story, then it seems reasonable to conclude that growth is a deficit-funded-foreign-born-healthcare story.3
It’s a bit of a mouthful, but it seems basically correct.
We’ve got a healthcare spending problem—a problem that also happens to be a major source of GDP—and we’ve relied on “foreign born” labor (and debt) to get our fix.
Without passing any judgment, Random Walk is just telling it like it is.
Open Border, now closed
Which brings us to the present: what are we going to do now that the supply of foreign-born workers is no longer set to “firehose”?
How are we going to feed our little “healthcare GDP and job-maker engine” without blowing wages out the wazoo?4
This too is no exaggeration: behold by far the most consequential policy shift of the new admin:
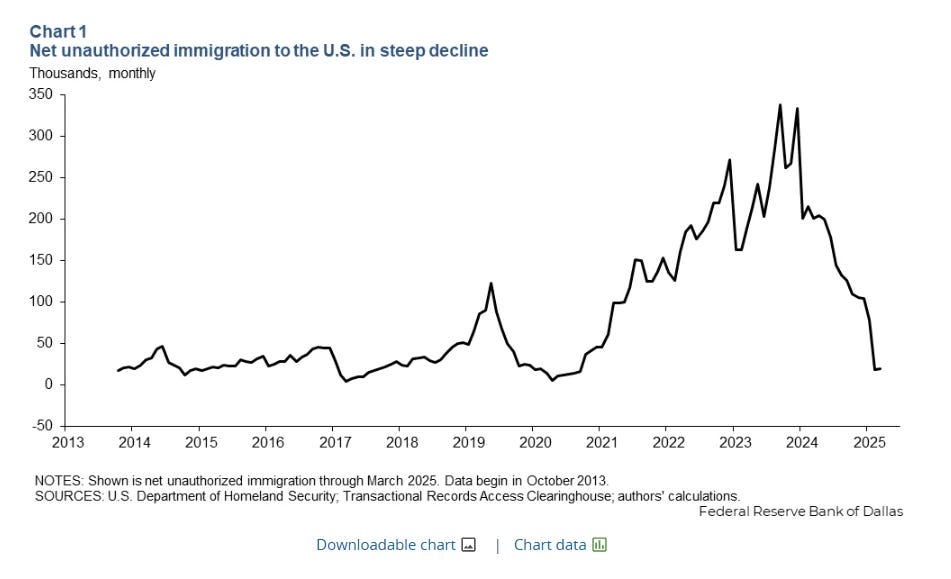
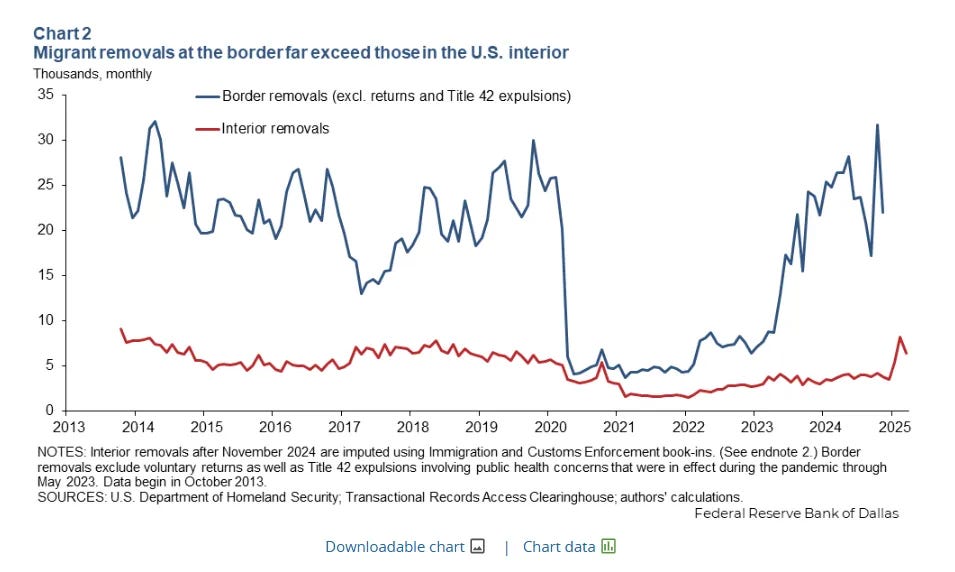
Historic levels of illegal immigration have abruptly collapsed, as immigration enforcement returns to the status quo ante.
Again, without assigning any judgement, it seems indisputable that the Biden admin facilitated an historic surge in illegal migration through non-enforcement of immigration law, while the Trump admin has done the opposite of that.
‘Native-born’ return?
The question now is where does job growth come from (and at what cost)?
For now, the early returns suggest mostly there isn’t much job growth, but perhaps there’s been some success at bringing “native born” workers off the bench:
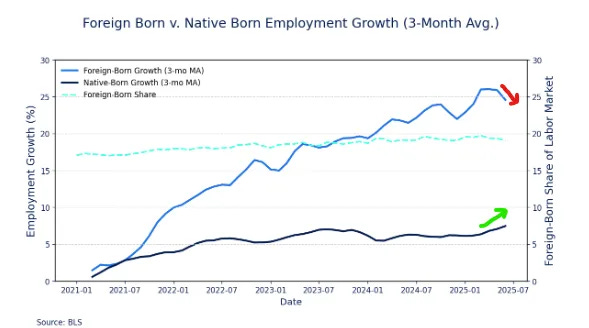
For basically the first time in three years, foreign-born job growth shrunk, while native-born job growth grew.
Now, I’m skeptical of month-over-month wiggles, so it’s going to take more convincing that closing the border has become a native-born job-maker, but time will tell.
For what it’s worth, there are some anecdotes of college-aged ski bums, stepping into the void.
Uncle Sam’s Immigrant Nursing Brigade, gone fishing?
But, back to healthcare specifically, because really, that’s the one that matters (and it’s where we started).
I mean, it’s no surprise that the oldest parts of the country have experienced the most substantial increases in healthcare jobs, and are also the most likely places to offer “visa support,” to fill those jobs.
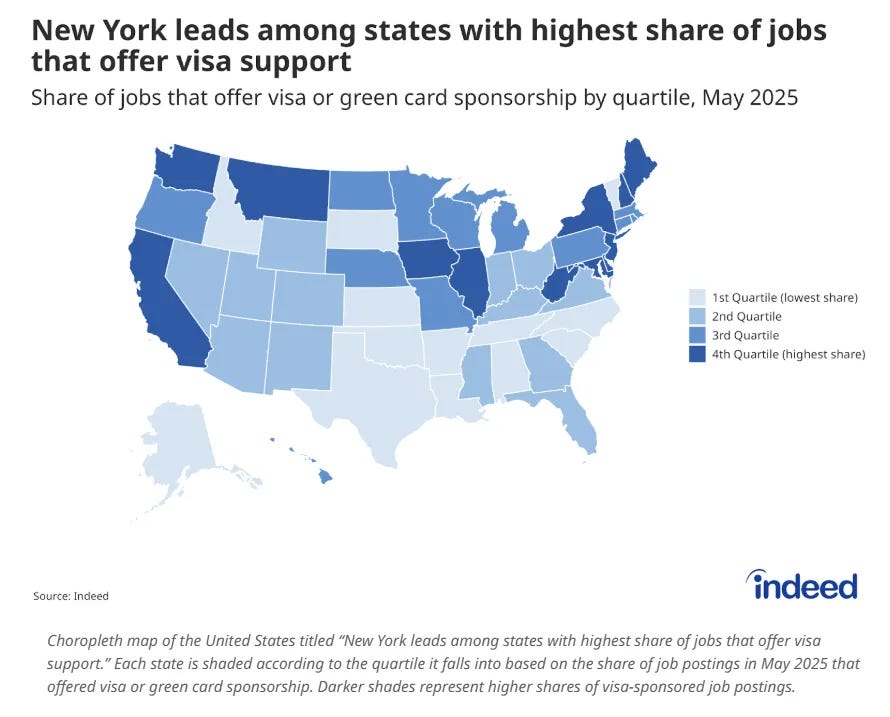
New York, California, NJ, and Illinois are demanding the sharpest increase in healthcare workers (especially home-health aids), and also happen to have the highest shares of job-postings offering “visa support.”5
It’s probably not a coincidence. Healthcare is job-growth, and job-growth is a foreign-born story. So, if you need healthcare workers, then you’re likely going to need visa-support.
As it turns out, medical jobs generally are far more likely to offer visa support:
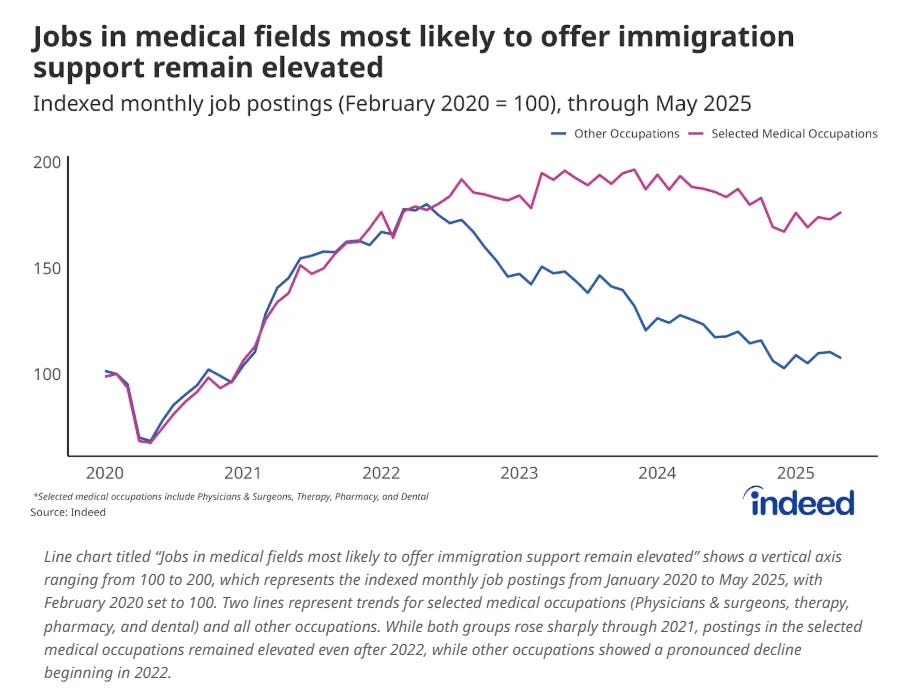
Medical job openings remain elevated, relative to other occupations.
As I’ve been saying, healthcare is in hiring mode, and healthcare hiring is a foreign-born game. But with the new sheriff in-town, what are we gonna do? We can’t stop buying healthcare, and we can’t keep importing people to do the work, but we also can’t pay even more for the few healthcare workers we have.
We need more healthcare workers, and we need ‘em cheap—but the international emporium of cheap healthcare workers is now closed. Sounds bad.6
We need healthcare YIMBY and we need it now
Well, I already told you what we’re gonna do: Healthcare Yimbyism.
You see, I’m going to posit that all this going overseas for doctors and surgeons and nurses is, in large part, just an arb on the relatively high cost of training healthcare workers domestically.
In this country, in order to be a doctor or a nurse, you first need to take on hundreds of thousands of dollars worth of debt, and a decade’s worth of indentured servitude. It’s an expensive, long-term commitment that’s full of uncertainty, and an absolute grind. And even if you make it through the gauntlet, the payback is high (because it has to be), and yet, because Uncle Sam is paying (and ROI has nothing to do with it), it’s not quite so high to really make it all worth the effort.
Little wonder we have a shortage of “qualified” healthcare workers, such that we have to tap international markets to fill the void. ‘Oh you got your medical degree in Pakistan (or whatever) [where training is a relative pittance]?! When can you start?’
I mean, if we’re willing to accept reciprocity from all over the world (which seems reasonable), then we should just admit that we don’t need all the hoops we jump through here (which, of course, we don’t).
The obvious and best solution to the healthcare-worker shortage is just make it easier for people to enter the business of healthcare, without first deciding to give up decades of their life to an absurdly difficult, expensive and uncertain obstacle course. There’s plenty of folks who’d like to “help people,” but because the path to doing something that sounds helpful (but is also relatively useless), like working at a not-for-profit (or something), is relatively cheap, they do that instead of healthcare.
And who can blame them? Entering the healthcare profession is like signing away a kidney for the privilege of sleepless nights, no control over your schedule, and endless bureaucracy and paperwork. Sounds awful.
Instead, we have something as dumb as a nursing shortage because, I shit you not, we have a shortage of nurses to train more nurses.
If YIMBYs were smart, they’d stop prattling about the fake housing shortage, and focus their attention where YIMBYism would actually make a massive difference for the better: healthcare. 7
Just rip it all out, root and branch.
Piecemeal won’t do it because it’s just a pile of bad regs plugging holes from bad regs plugging holes from bad regs. Whatever the negative consequences of an un-throttled industry, they can’t possibly be worse than what we have now (and what we have now is bankrupting us, so y’know, what choice do we really have)?
Other interesting reads
Dartmouth joins ivy league bond boom. Passing around the hat.
iCapital raises $820M at $7.5B valuation. iCapital provides software to wealth advisers etc. that helps offer retail access to alts. The rotation to privates continues apace.
The rise of ‘CV-Squared’. There are now continuation vehicles to take out continuation vehicles, which is what happens when companies stay private for longer (for better or for worse).
Former Citadel Quants raise $36M for Moment, a fixed-income trading and ops and platform. As capital markets (and credit markets especially) embrace a broader set of players and asset-types, the core technology needs to get leaner and smarter. You can’t have a more liquid market for private credit trading, for example, without the rails to facilitate custody, clearing, pricing, etc. Also, this is a good example of cross-pollination between asset classes generating a meaningful unlock.
JPM tells fintechs they have to pay up for data. This is a big change. Fintechs like Plaid, Paypal, Coinbase, etc. leverage bank customer data to drive core products and services, and they’ve done it for free. That JPM is charging for it is a big deal. The other part of this is regulation driven: the CFPB passed its ‘open banking’ rule that gives consumers the “right to their data,” including the right to permission it to other platforms. Banks are now saying, “we do all the work of collecting and keeping this data safe, so if we’re obligated to permission it, then we’re going to charge for it.”
Previously, on Random Walk
Private Credit and Insurance, two peas in a pod (reprise), and a chart dump on default rates

five charts on the rise of private credit in life insurance

Energy in 1776

It’s July 4th, so Happy Birthday America, and we’re going to keep it light and only semi-topical.


Random Walk is an idea company dedicated to the discovery of idea alpha. Find differentiated data, perspectives and people, and keep your information mix lively. A foolish consistency is the hobgoblin of small minds. Fight the Great Idea Stagnation. Join Random Walk. Follow me on twitter. Follow me on substack:

I’m not sure I’d call it a regulation, but it would also be critical to cap med-mal liability substantially, and perhaps create a specialized court system to adjudicate those claims.
Just to head off the inevitable “ohhh the horror of unregulated medicine—think of all the horrible things!” Look, when we shop for healthcare, no one is pulling licenses, certifications or degrees—we ask our friends, and/or we trust the institutional brand. We’d keep doing that. Plus, there are all kinds of important complicated things that we don’t require 15 years of school, like software engineering, for example, which includes a lot of the software that’s used in medicine. More broadly, just because ‘anyone can be a doctor’ doesn’t mean we’d trust anyone claiming to be a doctor, nor does it mean fraud, etc. suddenly becomes legal.
That picture was painted in stark relief when the pandemic “pulled forward” retirements, thereby exacerbating the “worker shortage,” causing wages to spike, leading to inflationary pressure, that was gradually brought to heel by an historic surge of “foreign born” workers (both legal and illegal). In other words, the Great Replacement is Real, Pro-Growth, and Deflationary aka The Open Border Saved the Economy.
This is the story at the margins. And no, immigrants don’t substitute for retirees or healthcare workers on a 1:1 basis, but they do perform a lot of healthcare work, a lot of work that healthcare workers might otherwise provide, and a lot of work that healthcare workers otherwise consume, like retail and food services.
Keeping in mind that “feeding it” isn’t really a good thing either. Deficit-funded eldercare that proceeds by acquirehire only is neither financially sustainable, nor culturally sustainable. It’s a bit of rock and a hard place, to put it mildly.
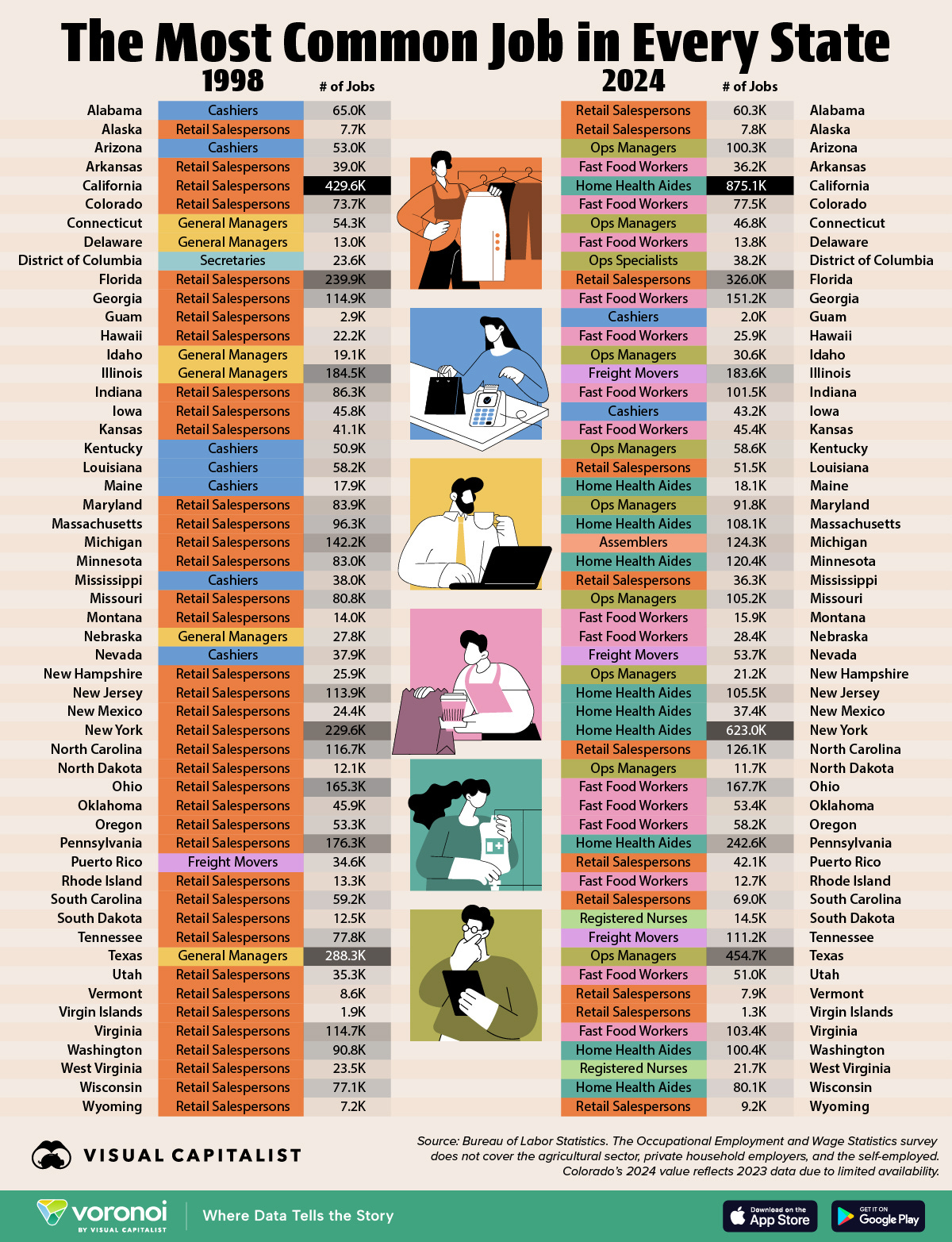
Another visual on the rise of Home Health Workers as the fastest growing profession
There’s already some evidence that wage pressure in services especially is rising.
Plus, income tax receipts grew 10%(!) yoy:

I’m not sure how else to explain a 10% jump in w2 taxes other than a jump in wages (unless there’s some mid-year cost-of-living increase I’m not aware of).
Instead, the same people who doggedly insist that unaffordable housing will become more affordable if we remove supply-side restrictions, also insist that unaffordable healthcare will become more affordable if we just restrict ALL the supply, and nationalize the industry instead. It’s almost like they’re not so much committed to Hayekian insights, as they are reallocating goodies more to their liking.
The US for some reason insists that you can only study to be a doctor, dentist, veterinarian, or lawyer after you complete 4 years of undergraduate college. Most of the rest of the world does not require this. That requirement burns years of time and huge amounts of money. It also shortens the length of time these professionals have to practice before retirement by 4 years reducing the overall work force. Really dumb.
“Look, when we shop for healthcare, no one is pulling licenses, certifications or degrees—we ask our friends, and/or we trust the institutional brand. We’d keep doing that. “
You know it takes months to switch jobs as a physician because that’s how long it takes the new employer to vet whether someone is safe to employ despite there being a national clearing house of strikes against physicians and states issuing and maintaining licenses for physicians.
This cultural change to happy go lucky health care will be a big one!